
CONGRESSIONAL WHITEPAPER – ADDRESSING THE KIDNEY TRANSPLANT SHORTAGE BY SUPPORTING LIVING DONOR FACILITATOR TRAINING PROGRAMS
Proposal:
Congress Can Enact Establish a Living Donation Facilitator Training Program for Advanced Chronic Kidney Disease Patients and Potential Living Donors, Enhancing Existing Medicare Policy and Saving Billions of Dollars.
Overview
More than 94,000 Americans are currently waiting for a kidney transplant, yet the supply of available organs continues to fall well short of demand. In 2025, the United States experienced the first decline this century in total kidney transplants because of a drop in deceased donor kidney donations. Even as the kidney discard rate improved and living donation increased slightly, the overall number of transplants declined, worsening the shortage facing patients who depend on transplantation to survive.
As documented in a KTC study of donation rates, with 21,856 deceased donor kidney transplants and 6,522 living kidney donor transplants occurring last year, 2025 was the first year in the 21st century that an isolated decline in deceased kidney transplants caused an overall decline in kidney transplants.[1] This is particularly startling as federal policy has relied on deceased kidney donations to address the waitlist, with the number of deceased donors increasing by over 170% over the past 20 years and the number of annual living donors remaining relatively stagnant.[2] To add further fuel to the crisis, JAMA Network Open estimates that as efforts are undertaken to add more patients pre-emptively to the waitlist in pursuit of positive health outcomes, approximately 2,800 additional kidneys would be required under a 10% waitlist expansion and more than 11,000 under a 50% expansion just to maintain current waitlist times.[3]
These points clearly demonstrate that a focus on discard rate improvement and deceased donor increases alone are insufficient; increasing living kidney donations must be part of the solution.
The Problem: The Kidney Transplant Crisis Is Growing
There Is A Shortage of Kidneys Currently Available:
Americans with End Stage Kidney Disease (ESKD) have two options: dialysis, which is an expensive and difficult treatment, or a kidney transplant. Yet, there is a significant shortage in America of kidneys available for transplant. While kidneys are available for transplant from both deceased and living donors, the available number of deceased donor kidneys will never meet this need. There are many more kidneys available from potential living donors and tens of thousands of living Americans would be willing to donate a kidney.[4] To date, however, Medicare has not leveraged its statutory and regulatory authority to expand living kidney donation.
Almost One Million Americans Have Kidney Disease:
The National Institutes of Health reports that as of June 30, 2025, 857,305 Americans were living with End-Stage Kidney Disease (ESKD).[5] There are two primary treatments for the disease – dialysis or kidney transplant. As of June 30, 2025, 560,230 Americans are on dialysis. Sadly, the United States now ranks 27th in the world in transplants for people on dialysis.[6]
Medicare Spending on Kidney Disease Is Very High and Rising:
Medicare spends a massive amount to treat ESRD patients on dialysis. The National Kidney Foundation reports that Medicare each year spends more than $130 billion (24% of overall spending) on patients with kidney disease and ESRD, which affects 1% of Medicare beneficiaries and accounts for 7% of total Medicare spend.[7] Similarly, the NIH estimates that in 2021, 13.5% of the approximately 23.9 million Medicare fee for service beneficiaries over 66 years old had a diagnosis of Chronic Kidney Disease (which includes ESRD), accounting for nearly one-quarter (24.1%) of total Medicare spending – an estimated $76.8 billion dollars. Within that group, approximately two thirds of the cost ($52.3B in 2021) was spent on care for ESRD beneficiaries.
While Medicare spending on kidney disease is immense, it is also important to note that private insurers are also statutorily required to pay for transplants and kidney disease. This statutory requirement is important to highlight not only because it speaks to the significant healthcare expenditures in this space, but also because any Medicare requirement related to kidney transplants also naturally brings along commercial insurer payments as well.
More Support Is Needed:
Unfortunately, while living donation has been proven to be safe, living donation rates have stagnated over the past 25 years between approximately 5,200 and 6,600 donations per year. Living donor organs have long been considered preferable by practitioners for two reasons: (1) there will never be sufficient deceased organs available to meet patient needs;[8] and (2) living donor kidneys last nearly twice as long as deceased donor kidneys,[9] producing far better recipient health outcomes and avoiding individuals returning to the waitlist for a second transplant. Living donation also creates the best opportunity for a preemptive kidney transplant. Preemptive transplants are associated with the highest survival rates, improvements in quality of life and significant cost savings by avoiding the high expenses of the months immediately before and after dialysis initiation, which can exceed $15,000 per month.[10]
Policy makers have more recently begun to address the flat lined rate of living kidney donations, but their focus has largely centered around financial support for living donors. While absolutely essential, this policy focus does not acknowledge the fact that a significant percentage of the adult population are already very willing to donate their kidney to a friend or family member. A survey conducted by the Mayo Clinic in 2013 of over 1,000 adults, showed that 84% of respondents said that they would consider donating a kidney to a close friend or family member in need and 49% indicated that they would be willing to do the same for someone that they have never met. This is referred to as an altruistic or non-directed donation.[11] A more recent survey of over 800 US adults (age 25-65) conducted in 2021 and published in 2024 demonstrated that almost 87% would consider becoming a living kidney donor. [12]
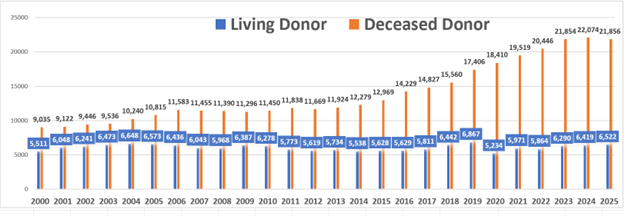
In light of the evidence suggesting that so many Americans are willing to serve as a living kidney donor, why have living kidney donor transplant rates stagnated over the past 25 years as the chart below of OPTN data showing deceased and living kidney transplants on an annual basis from 2000 through 2025 clearly demonstrates. Living kidney donors save lives, yet there is no specific or coordinated federal support system to help patients find a donor or guide potential donors through the complex transplant process from start to finish.
Millions Of Americans Are Willing to Donate But The System Lacks Support:
Patients are expected to find a donor on their own and don’t have the resources to turn to their networks to ask or recruit a willing living donor. In turn, potential donors are not being recruited or provided access to opportunities to donate to those in need. Moreover, potential donors who step forward face a complex and confusing evaluation process. Only a small fraction of potential donors who begin the evaluation process ultimately complete the donation. Many fall away not because they stop wanting to help, but because the system makes it too difficult to follow through. Research underscores how steep that drop off can be. That gap between willingness and completion is where lives are being lost.
One reason for this stagnation is that Medicare regulations work against advancing living donation, rather than aiding those with ESRD and advanced CKD in identifying living donors and assisting those potential living donors in pursuing the complex and costly process of donating.[13] Many prospective donors report difficulties in communications with transplant centers, trouble navigating the potential financial costs (travel, time away from work, and dependent care) resulting from donation, or the difficulties navigating the multiple days of clinical testing. As a result, while some percentage of candidates may prove ineligible to donate for medical reasons, the vast majority of candidates drop out due to the logistical difficulties. A study published in Transplantation Direct in 2021 using data from ten transplant programs found that only 29% of potential living donors evaluated were able to actually serve as a living kidney donor despite using an independent advocate provided by the transplant center.[14] Many of the barriers to serving as a living kidney donor are reviewed in an abstract from the American Society of Transplant meeting in 2025 entitled: “Donor Detours: Understanding the Barriers to Living Kidney Donation.”[15] The transplant program at the University of Illinois at Chicago received 320 living donor referrals in CY2024. The abstract shows that while the majority of these referrals were closed as a result of medical and psychological contraindications due to hypertension or inadequate kidney function, these were closely followed by patient choice as the reason. With adequate support navigating the donation process, more patients would likely follow through.
The Solution
Kidney Transplant Is the Optimal Treatment – Both from a Health and Fiscal Perspective:
Kidney transplant is the “optimal treatment” for those facing or on dialysis. The March 2026 MedPAC Report to Congress notes in Chapter 5: “Kidney transplantation is widely regarded as a better ESRD treatment option than dialysis in terms of patients’ clinical outcomes and quality of life. In addition, transplantation is associated with lower Medicare spending.”[16] “Although not a cure for kidney disease, a transplant can help a person live longer and improve quality of life. On average, patients experience 14 to 16 years of function from a kidney from a living kidney donor, while few people survive more than a decade on dialysis.”[17] The health benefits of transplant are further enhanced by the cost savings. A recent private study, using Congressional Budget Office scoring conventions, has estimated that each kidney transplant saves the Medicare program $800,000 over ten years.[18] Doubling the number of new living donor transplants over the next decade would reduce Medicare spending by $6.6 billion. By having transplant hospitals train Living Kidney Transplant Facilitators, the number of living donor kidney transplants could increase from 6,000-6,500 to 12,000-13,000 annually, producing an estimated $300,000 in savings per patient by year 5 and $800,000 per patient over 10 years.
Deceased Donations Were Relied on But are Now Falling:
From 2000 to 2024, the number of deceased donor kidney transplants in the U.S. increased with a more significant and sustained increase from 2013 through 2024. This improvement was initiated by the passage of the National Organ Transplant Act (NOTA) in 1984 which established the Organ Procurement and Transplantation Network (OPTN) and the United Network for Organ Sharing (UNOS). The OPTN implemented national allocation policies to standardize organ distribution, reduce waiting times and increase matching efficiency. By the early 2000s, Donation after Circulatory Death (DCD) expanded to increase the recovery of organs from deceased donors. Public awareness and donor registrations grew as a result of federal and state educational campaigns, alongside systemic improvements. These regulatory and safety measures increased public trust in donation, while the availability of real-time data analytics from the OPTN helped focus attention on areas for improvement. A donor can be declared deceased after circulatory death or brain death, and the movement towards recovering more kidneys after just circulatory death and not after brain death has been marked, increasing from approximately 2% of deceased donors in 2000, to 49% of donors in 2025. Donation after circulatory death now accounts for 45% of all deceased donor kidney transplants.[19]
Unfortunately, in 2025 we witnessed a departure from this trend. On January 14, 2026, the Kidney Transplant Collaborative (KTC) released a new report, Losing Transplants for All the Wrong Reasons. The report reveals a clear and unprecedented shift in 2025. For the first time this century, we saw an annual isolated decline in deceased donations and deceased donor kidney transplants, even while living donor kidney transplants increased and the kidney discard rate declined. Even more alarmingly, this deceased donor decline led to an aggregate decline in kidney transplants in 2025.
Based on national data and the timing of events, KTC identifies three likely drivers of this decline. First, public confidence has been shaken following widely publicized cases involving attempted organ recovery in patients who later showed signs of life. Second, donor withdrawal rates have increased as individuals remove themselves from registries. Third, OPOs may be operating more cautiously in response to investigations, legal exposure, and public scrutiny, particularly in Donation After Circulatory Death cases that historically supported transplant growth. While oversight matters, the environment created by these incidents appears to have shaken public trust and altered behavior across the broader health system.
In 2020, only 10% of potential deceased donors younger than 76 years old with an inpatient death and organs suitable for transplant actually served as organ donors. Given this unrealized potential, both Congress and CMS took action. More specifically, Congress began a series of oversight hearings into OPO operations, The OPTN which coordinated the OPOs, and the high discard rates of recovered organs. In parallel, CMS in December 2020, issued a final rule focused on improving OPO performance, threatening to decertify the lowest performing OPOs unless deceased donor organ recoveries and transplantation rates increased.
On March 11, 2026, CMS issued new guidance to address these concerns by strengthening public trust in the organ donation system. This guidance clarifies and reinforces the responsibilities of both the OPOs and donor hospitals by ensuring that patients receive full and complete medical care irrespective of potential donor status along with providing families with adequate time to make informed decisions regarding organ donation for their loved one without any coercion.[20]
While congressional oversight of OPO practices is critical to restoring trust in the deceased donor system, Congress should return to the original goal of its investigation and refocus on how our country can increase kidney transplants. Second, while the efforts underway to restore trust and confidence in the United States organ donation and transplantation system are critical, stakeholders must recognize that in the short term the oversight efforts have led to a decrease in deceased donors. Given that reality, the only immediate solution to this crisis is an increase in living kidney donation.
Living Donors Are The Answer:
Congress could clearly establish the operation of living donor transplant facilitator training programs as a transplant hospital reimbursable activity. This update would create specific trainers (paid for by Medicare) to teach and support living kidney transplant facilitators (volunteers – friends and family of recipients and living donors) to help oversee the search for and assist in identifying a potential living donor, and then work with the potential living donor as the donor’s advocate through the pre-transplantation, transplant surgery and post-transplantation process. The legislation would allow the time and cost of the hospital-based trainers to be reimbursed as a reasonable cost on the transplant hospital cost report. The program would be optional for transplant hospitals, but given that these activities would be appropriately reimbursed (which they are not today) transplant hospitals are highly likely to participate to increase the number of living donors, increase revenue responsibly, and save both thousands of lives and billions of Medicare dollars.
The Living Kidney Transplant Facilitator Program Solution:
Congress could enact legislation clarifying existing regulation in legislation that would further advance living donation across the nation. More specifically, Congress should allow Medicare to reimburse transplant hospitals for training living donor facilitators who help patients identify potential donors and guide those donors through the transplant process.
More specifically, Congress could amend the living donor provisions of the Medicare statute to create a specialized Living Kidney Transplant Facilitator training program for ESRD and advanced CKD patients who are potential transplant recipients and for the prospective living donors who are prepared to help them. The legislation would allow (but not mandate) transplant program staff to provide training services to allow navigators – families, friends and community members dedicated to helping potential kidney transplant recipients – to help potential recipients identify living donors and then to assist potential living donors in getting through the transplant process. By clarifying that the hospital training activities would be deemed reasonable costs eligible for reimbursement through the hospital cost report, transplant programs could hire the needed staff to train the community-based facilitators to assist potential recipients identify a living donor and then support that living donor through the transplant process, thus increasing the number of living donor transplants, improving health outcomes, and saving the Medicare program significant sums.
A more detailed explanation of the proposed solution follows:
Numerous clinical studies have demonstrated that transplant facilitator interventions by friends, family, and aligned community members committed to supporting recipients could materially increase living donor transplantation. Providing transplant hospitals with the staff to train transplant facilitators – friends and family of the potential recipient in identifying a living donor and training a similar transplant facilitator to assist the potential donor to help them complete the complex pre-donation and donation process, would materially increase the number of living donations from today’s stagnant rates.[21]
In addition to improving donor identification rates, facilitator training programs lead to transplant facilitators helping donors and recipients plan transplant surgeries – enabling hospitals to schedule surgeries in advance, improving operating room efficiency and optimizing clinical resources. Planned living donor transplants allow both recipients and donors to undergo surgery under ideal conditions, reducing cancellations and improving outcomes.
A growing body of clinical evidence demonstrates that transplant facilitators materially increase the number of successful living donor transplants, often at minimal cost and with rapid impact. Programs that introduce a trained facilitator, someone who guides recipients and their families in identifying potential donors and developing the language needed to make the ask, have produced dramatic improvements. Equally significant is the impact facilitators have on individuals who volunteer to become living donors but face a complex evaluation process that deters even the most motivated candidates. Facilitators help prospective donors navigate medical testing, coordinate appointments, and overcome logistical barriers that often have nothing to do with medical fitness. Several non-profit programs across the country, for example, have demonstrated that structured outreach and donor navigation can support hundreds of additional living donor transplants each year.[22] [23] [24] Yet, despite these successes, Medicare provides no clear reimbursement mechanism for transplant hospitals to support facilitators, even as it funds far higher costs associated with deceased organ acquisition, including high-priced organ recovery logistics and private aviation transport for recovered kidney organs. Establishing facilitator training expenses as reimbursable organ acquisition costs would align federal policy with existing practice and deliver a cost-effective, scalable solution capable of offsetting the sudden decline in deceased donation.
The Living Donor Facilitator Training Program In Action:
A Proven Method:
Expecting ESRD patients to find living donors on their own is often unrealistic. Studies, however, have shown that when a transplant program trains a facilitator to assist dialysis patients and arm them with the language to ask someone to be their living donor, identify potential donors, and even in some cases initiate the outreach for the potential recipient, the likelihood that a living donor can be found significantly increases.[25] By providing this support for those needing a transplant at an early stage, the challenges that the living donor faces, once identified, to completing a living kidney donor transplant can be overcome inexpensively and efficiently.[26]
At the University of Alabama Birmingham, the transplant hospital trained facilitators in an 8 week advocacy and educational course, instructing the facilitators on engaging and educating the family, friends and social network of the prospective recipient about the prospects of living donation. Following the “advocacy” training, the facilitator worked with the recipient’s networks to identify the living donor (in some cases actually making the ask of the potential living donor rather than having the recipient ask). Following agreement, the facilitator applied their training to guide the living donor through the medical testing process and through the transplant surgery. In addition to the advocacy training, the facilitator also received “systems training” on the “how, why and when” of the medical testing journey, which they put to work in regular contact with the prospective donor, including before each medical visit, to ensure the living donor made it through the process.
Similarly, at Johns Hopkins University, training was focused on giving facilitators the skills to seek out the living donor, thereby “separating the advocacy from the patient.” By providing intensive training in transplant, how to initiate the discussion with living donors, building the networks, and sharing success stories, the facilitators not only were able to directly identify living donors for a recipient, but the recipients grew more comfortable participating in the process.
The results of these programs were stunning. For example, the Johns Hopkins “Champions” program reported a massive increase in recipients identifying living donors following the transplant hospital training facilitators to provide assistance to potential recipients by teaching the facilitators the language to use in asking individuals to consider living donation, providing educational materials on the risks or being a living donor, and sharing effective strategies for outreach to potential living donors. A peer reviewed study of the program found:
Current educational modalities or interventions do not adequately meet the needs of patients who would like to pursue and identify live donors. Education alone is not sufficient to decrease the anxiety and fear associated with approaching potential donors. In this trial, LDCs successfully helped increase comfort and decrease concerns associated with approaching a live donor. A dramatic proportion of participants (almost 50%) identified live donors, compared with matched controls for whom no live donors were identified.[27]
Providing those eligible for transplant with a facilitator trained by the transplant hospital using the Hopkins protocols to assist in identifying living donors would add a massive number of new transplants to the system, driving huge savings at a trivial cost.
Assisting Potential Donors:
Similarly, giving individuals who volunteer to be considered for living donation a facilitator trained by the transplant hospital to help the potential living donor through the extensive medical testing and eventual surgery has also been shown to multiply the prospects of living donation. In one study at the University of Alabama Birmingham (UAB):
[i]implementation of a [Living Donor Facilitator] Program was associated with a 9-fold increased likelihood of living donor screenings and a 7-fold increased likelihood of having an approved living kidney donor among program participants compared to standard of care.”[28]
Again, providing a potential donor with a facilitator would cost a trivial amount, for massive returns. As noted above, today 93 of every 100 potential living donors willing to be screened never make it to donation. Adding facilitators could radically change that figure, and increase living donation an estimated 7 times, so that 49 of the 100 candidates complete the donation process.
Including Transplant Hospital Costs for Training the Facilitators on the Cost Report Should be Non-Controversial:
The concept of including the transplant hospital costs for training facilitators within the transplant center cost report is not novel and fits comfortably within the mainstream of costs that are currently being reimbursed by Medicare through the cost reports. Under applicable regulation[29] and CMS guidance,[30] organ acquisition cost reimbursement today pays tissue typing, donor and beneficiary evaluation, organ preservation and perfusion costs, OPTN fees, surgery costs to recover deceased donor organs, procurement costs charged by other organizations in the system, and deceased donor organ transportation costs. Not inappropriately, the transportation costs include private jet transport of deceased donor organs, which can cost tens of thousands of dollars per donation. Yet, when it comes to living donors, there is no regulation or guidance that would allow a transplant hospital to put the costs of training the community-based facilitators on the cost report, even though it may be a material to the transplant happening. And importantly, it is only the hospital employees doing the training and ongoing follow up with the facilitators that would be on the cost report – the facilitators are volunteers whose time would not be charged to the program.
The reimbursement of acquisition costs on the cost report began in 1974, and has been expanded over the years. Since 1978, all organ preservation and perfusion costs have been designated as “Pass Through Costs” and are payable through the cost report, as are other direct and indirect costs associated with operating a transplant program. In contrast, CMS regulations prohibit payment for travel, room and board expenses incurred by the living donor or recipient. Ironically, Medicare is already indirectly paying for hidden facilitation costs, along with numerous other costs that transplant hospitals may not directly bill for, if those services are provided by a third party. There are several organizations in the U.S. that match living donors or create donor chains that charge transplant programs an acquisition fee for procuring the donation, which in turn the transplant center includes on the cost report. Embedded in the acquisition fee can be facilitator costs, travel costs, and even legal support costs. Thus, given that Medicare may, in some cases, already be paying for these costs indirectly, it makes sense for Medicare to pay for them directly as well.
Recognizing the modest costs associated with living donor facilitator training would require only a fraction of that investment. Incorporating these facilitator training expenses into the Organ Acquisition Cost framework would be a logical and efficient extension of existing Medicare policy, ensuring that relatively small expenditures translate into far greater numbers of successful transplants and lives saved.
In comparison to paying thousands of dollars for private jet transportation, paying for the few hundred dollars it will cost for a hospital-based trainer to train a facilitator to assist in arranging a living kidney donor transplant is more than reasonable. Finally, there is a significant need for further steps to increase living donation as a result of an alarming trend overtaking the transplant community. More specifically, in response to media reports of irregularities in deceased donation organ recovery, tens of thousands of Americans have recently (in 2025) withdrawn their consent to be a deceased donor[31] and deceased donation rates are dropping. Thus, as the availability of deceased donor organs declines due to external events, it is even more imperative to ensuring living donors can fill in the gaps.
Implementing these modest changes would likely double the number of living donors within a few years, improving outcomes, reducing the waitlist, and saving Medicare an estimated $6.6 billion over ten years. These reforms could result in more than 40,000 kidney transplants annually—12,000 to 13,000 from living donors alone—representing one of the few policy changes in healthcare that simultaneously improves survival, enhances quality of life, and reduces long-term federal spending. The establishment of living donor transplant facilitator programs in transplant centers nationwide would ensure that every American in need of a kidney has a timely path to transplant.
[1] insights.unos.org/OPTN-metrics/
[2] kidneytransplantcollaborative.com/wp-content/uploads/KTC-Dec-2025-Deceased-Donor-Report-UPDATED.pdf
[3]jamanetwork.com/journals/jamanetworkopen/fullarticle/2831868?utm_campaign=articlePDF&utm_medium=articlePDFlink&utm_source=articlePDF&utm_content=jamanetworkopen.2025.1665
[4] www.kidneymedicinejournal.org/action/showPdf?pii=S2590-0595%2823%2900206-6
[5] www.niddk.nih.gov/about-niddk/strategic-plans-reports/usrds/esrd-quarterly-update
[6] usrds-adr.niddk.nih.gov/2025/end-stage-renal-disease/11-international-comparisons
[7] https://www.kidney.org/get-involved/advocate/legislative-priorities/federal-investment
[8] Matas AJ, Montgomery RA, Schold JD. The Organ Shortage Continues to Be a Crisis for Patients With End-stage
Kidney Disease. JAMA Surg. 2023 Aug 1;158(8):787-788. doi:jamanetwork.com/journals/jamasurgery/fullarticle/2805308 (“Given that only about 1% of deaths occur in a manner suitable for organ donation, there appears to be no possibility that any further increase in deceased donation will be sufficient to eliminate the shortage. Similarly, there is currently a considerable emphasis on minimizing the number of deceased donor kidneys recovered but not transplanted; however, at best, that alone might result in approximately 2000 more transplants per year, a mere dent in the problem.”).
[9] www.kidney.org/kidney-topics/becoming-living-donor
[10] jamanetwork.com/journals/jamanetworkopen/fullarticle/2797907
[11]newsnetwork.mayoclinic.org/discussion/mayo-clinic-poll-shows-half-of-americans-would-consider-donating-a-kidney-to-a-stranger/
[12] www.kidneymedicinejournal.org/action/showPdf?pii=S2590-0595%2823%2900206-6
[13] D. Cholin LK, Schold JD, Arrigain S, Poggio ED, Sedor JR, O’Toole JF, Augustine JJ, Wee AC, Huml AM. Characteristics of Potential and Actual Living Kidney Donors: A Single-center Experience. Transplantation. 2023 Apr 1;107(4):941-951. doi: pubmed.ncbi.nlm.nih.gov/36476994/
[14] pmc.ncbi.nlm.nih.gov/articles/PMC8078331/pdf/txd-7-e689.pdf
[15] www.amjtransplant.org/action/showPdf?pii=S1600-6135%2825%2901926-4
[16] www.medpac.gov/wp-content/uploads/2026/03/Mar26_Ch5_MedPAC_Report_To_Congress_SEC.pdf
[17] Medicare Program; Alternative Payment Model Updates and the Increasing Organ Transplant Access (IOTA) Model, 89 Fed. Reg. 96280, 96294 (December 4, 2024).
[18] The Moran Company, The Living Organ Volunteer Engagement (LOVE) Act: Fiscal Implications (March 15, 2024), available from author.
[19] jamanetwork.com/journals/jama/fullarticle/2845586
[20] www.cms.gov/files/document/qso-26-05-opo-original-release-date-2026-03-11-pdf.pdf
[21] Federal law and regulation requires transplant programs to have adequate support for living donors, 42 C.F.R. § 482.94, including having on staff an “independent living donor advocate team.” 42 C.F.R. § 482.98(d). While transplant hospitals do an excellent job at assisting the living donor through the surgical process, there is no federal program or Medicare regulation addressing living donation before a living donor arrives at a transplant hospital.
[22] kidneysforcommunities.org
[23] www.americantransplantfoundation.org
[24] renewal.org
[25] Garonzik-Wang JM, Berger JC, Ros RL, Kucirka LM, Deshpande NA, Boyarsky BJ, Montgomery RA, Hall EC, James NT, Segev DL. Live donor champion: finding live kidney donors by separating the advocate from the patient.
Transplantation. 2012 Jun 15;93(11):1147-50. doi: 10.1097/TP.0b013e31824e75a5. PMID: 22461037; PMCID: PMC3374007.
[26] See also Killian AC, Carter AJ, Reed RD, Shelton BA, Qu H, McLeod MC, Orandi BJ, Cannon RM, Anderson D, MacLennan PA, Kumar V, Hanaway M, Locke JE. Greater community vulnerability is associated with poor living donor navigator program fidelity. Surgery. 2022 Sep;172(3):997-1004. doi: 10.1016/j.surg.2022.04.033. Epub 2022 Jul 10. PMID: 35831221; PMCID: PMC9633042 (“The Living Donor Navigator (LDN) Program helps patients with end stage kidney disease identify living kidney donors and helps living donors navigate the complex evaluation process. LDN participants have demonstrated a 9-fold increased likelihood of donor screening and 7-fold increased likelihood of donor approval compared to nonparticipants”).
[27] Id.
[28] Locke, J., et al. Enhanced Advocacy and Health Systems Training through Patient Navigation Increases Access to Living Donor Kidney Transplantation, Transplantation. 2020 Jan; 104(1): 122–129. doi:
10.1097/TP.0000000000002732.
[29] 42 C.F.R. § 413.402.
[30] CMS Pub. 15-1, Ch 31 §3101.
[31] https://www.newsweek.com/thousands-remove-organ-donor-registries-nyt-coverage-2109940