More than 857,000 Americans are living with End-Stage Kidney Disease, and over 560,000 are on dialysis — an expensive, exhausting treatment that, for most patients, is a way to stay alive while they wait for a transplant that may never come. The waitlist now exceeds 94,000 people and grows every year. In 2025, just over 28,000 transplants were performed nationwide. The average wait is three to five years.
The waitlist is growing faster than the number of people receiving a transplant.
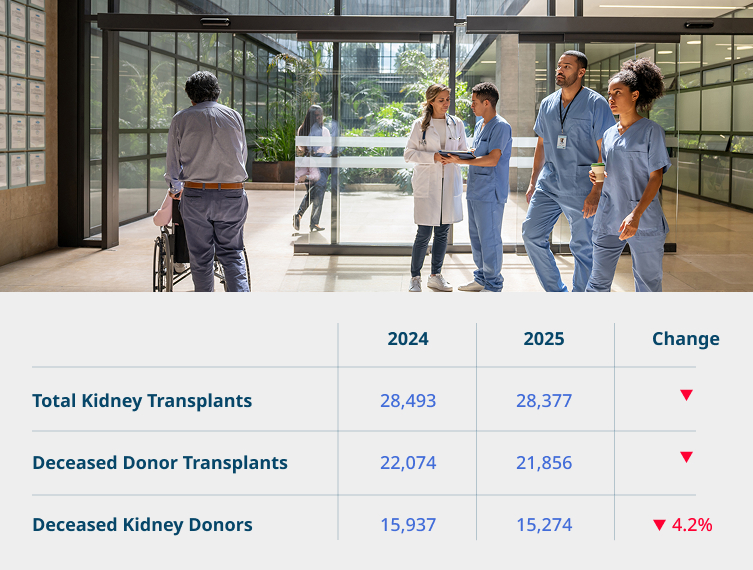
Sources: NIH / USRDS; OPTN National Data; KTC January 2026 report.
An Alarming New Trend
In 2025, kidney transplants declined for the first time this century outside of a pandemic year.
Kidney Transplant Collaborative was the first to document this trend, in a report published in January 2026.
It is the first time this century that deceased donations have fallen in isolation, not as part of a recession, a pandemic, or a broader policy shift. Rigorous oversight of the deceased donor system remains essential, but the consequence is clear: the deceased donor pipeline cannot be counted on to close the transplant gap. Demand keeps growing. Supply just shrank.
Deceased donor transplants more than doubled this century. Living donation barely moved.
Since 2000, deceased donor transplants have grown by more than 170% from roughly 8,100 per year to over 21,000. Living kidney donors have held essentially flat, oscillating between 5,200 and 6,600 per year.
It is not for lack of safety: living donor kidneys last nearly twice as long as deceased donor kidneys, and recipients live longer and healthier lives. And it is not for lack of willing donors. A Mayo Clinic survey found that 84% of respondents would donate to a friend or family member, and 49% would donate to a stranger. A 2024 national survey found 87% would at least consider it.
The willingness is there. The system isn’t built to convert it.
The Hidden Bottleneck
Of every 100 Americans who volunteer to be a living donor, only 7 make it to surgery.
Published research shows that out of every 100 potential living donors who complete an initial screening, only seven ultimately donate. Most do not drop out because they are medically unfit. They drop out because the process is long, fragmented, and uncoordinated — blood draws, crossmatch tests, medical and psychosocial evaluations, imaging, lifestyle requirements, and logistics spread over months and multiple specialists. Motivated volunteers give up. Recipients never learn how to ask.
Medicare has the power to fix this. Today, it doesn’t.
“Medicare will reimburse a private jet to fly a deceased donor kidney across the country. It will not reimburse the trained facilitator who could help a living donor get to surgery in the first place.”
Cholin et al., Transplantation, 2023.
What This Costs America
Medicare spends more than $130 billion a year on kidney disease. Every transplant saves roughly $800,000 over a decade.
Medicare spends more than $130 billion per year on patients with kidney disease, nearly a quarter of all Medicare spending. End-Stage Kidney Disease alone affects just 1% of beneficiaries but accounts for roughly 7% of total Medicare spend, driven overwhelmingly by dialysis.
Using CBO scoring conventions, each additional kidney transplant saves Medicare about $300,000 by year five and $800,000 over ten years. Patients who receive a living donor kidney experience an average of 14 to 16 years of kidney function; few patients survive even a decade on dialysis.
Every living donor transplant we fail to facilitate is a life cut short and hundreds of thousands of federal dollars spent on dialysis that wasn’t necessary.
Sources: National Kidney Foundation; NIH; The Moran Company (2024).
We know what the problem is. We also know what to do about it.
Studies from Johns Hopkins and the University of Alabama at Birmingham demonstrate that a trained transplant facilitator program dramatically increases completed living donor transplants. KTC has built a policy roadmap around that evidence enactable by Congress or by executive action.